What Is A Perfusionist?
A Perfusionist — formally known as a Clinical Perfusion Scientist — is a specialised healthcare professional whose main responsibility is the operation and maintenance of the cardiopulmonary bypass (CPB) machine, commonly referred to as the heart-lung machine. The profession emerged in the 1950s alongside the development of open-heart surgery; the first successful CPB-supported operation in the UK was performed in 1958.
Predominantly based in the cardiac operating theatre, the perfusionist's core role is to temporarily take over the function of the patient's heart and lungs during surgery. The CPB machine provides continuous blood flow to the body, oxygenates the blood, removes carbon dioxide, and regulates the patient's temperature — allowing the cardiac surgeon to operate on a still, bloodless heart. The perfusionist must continuously monitor and adjust flow rates, blood gases, haematocrit, electrolytes, anticoagulation, and temperature throughout the procedure.
Beyond cardiac surgery, perfusionists are also involved in extracorporeal membrane oxygenation (ECMO) — both venoarterial (VA) and venovenous (VV) — for patients with severe heart or lung failure. They may also prepare platelet-rich fibrin (PRF) products for wound healing, operate cell salvage machines, and assist with ventricular assist device (VAD) implantation. In the UK, there are approximately 300 practising perfusionists, all registered with the College of Clinical Perfusion Scientists of Great Britain and Ireland.
How To Become A Perfusionist
Example Adult Cardiac Procedures Requiring CPB
- Coronary Artery Bypass Graft(s)
- Atrial Myxomas
- Tricuspid Valve Repair
- Mitral Valve Repair / Replacement
- Aortic Valve Replacements
- Dissections / Aneurysms / Trauma of the Aorta
- Lung Transplant
- Heart Transplant
- Aortic Root Replacements
Heart Lung Machine
Operation of the heart-lung machine is the primary role of a Perfusionist. Modern heart-lung machines — such as the LivaNova S5 — are sophisticated medical devices that serve as the engineering platform for cardiopulmonary bypass. During each operation, sterile, single-use disposable equipment is assembled onto the machine and primed with a crystalloid solution (typically Hartmann's solution or Plasmalyte) to create a functional extracorporeal circuit.
The basic components of the bypass circuit include a venous reservoir, arterial pump, membrane oxygenator with integrated heat exchanger, arterial line filter, and a cardioplegia delivery system. Additional components may include haemoconcentrators (for ultrafiltration), in-line blood gas monitors, and venous oximetry sensors. The perfusionist is responsible for assembling, priming, de-airing, and operating this entire circuit — making real-time clinical decisions throughout the operation.
Venous Reservoir
Venous reservoirs collect blood drained from the patient via the venous cannula(e) placed in the right atrium or vena cavae. There are two types: open (hard-shell) and closed (soft-shell/collapsible bag) reservoirs.
Open reservoirs are the most widely used configuration in UK practice. They contain defoaming agents (typically polypropylene mesh coated with anti-foam compound) and integrated mesh filters to minimise gaseous and lipid microemboli from the surgical field entering the patient's circulation. Key advantages of open reservoirs include superior air-handling capability, compatibility with vacuum-assisted venous drainage (VAVD), and simplicity of operation — they do not require a separate system to manage cardiotomy suction blood.
Closed reservoirs offer certain theoretical advantages: better maintenance of sterility, a smaller blood-contact surface area (which produces less of an inflammatory response to cardiopulmonary bypass), and reduced haemodilution. However, they are more complex to manage — particularly with regard to air detection and handling — and require a separate cardiotomy reservoir for managing surgical field suction blood. For this reason, open reservoirs remain the standard of care in most UK cardiac centres.
Pump
There are two main types of arterial (blood) pumps used on the heart-lung machine: roller pumps and centrifugal pumps.
Roller pumps are positive displacement pumps that propel blood through flexible PVC tubing using two rollers mounted on a rotating arm. The rollers compress the tubing in a peristaltic motion, creating forward flow. Roller pumps deliver a known, predictable flow for any given RPM (determined by tubing size and rotational speed), making them straightforward to calibrate. They have been the workhorse of cardiac perfusion since the earliest days of open-heart surgery. However, they can generate high pressures if the outflow becomes obstructed and may cause some degree of haemolysis (red blood cell damage) due to the compressive forces on the tubing.
Centrifugal pumps use a magnetically driven impeller (rotating cones or vanes) inside a polycarbonate housing. Rotation generates a vortex that creates a pressure differential — drawing blood in through a central inlet and expelling it from a peripheral outlet via centrifugal force. Centrifugal pumps are pressure-dependent rather than volume-dependent, meaning they cannot generate dangerously high pressures against an obstruction (they will simply stop displacing blood). This is considered a safety advantage. They also produce less haemolysis at higher flow rates and are the pump of choice for ECMO circuits. However, they require continuous flow measurement via an in-line flow probe, as output varies with preload and afterload.
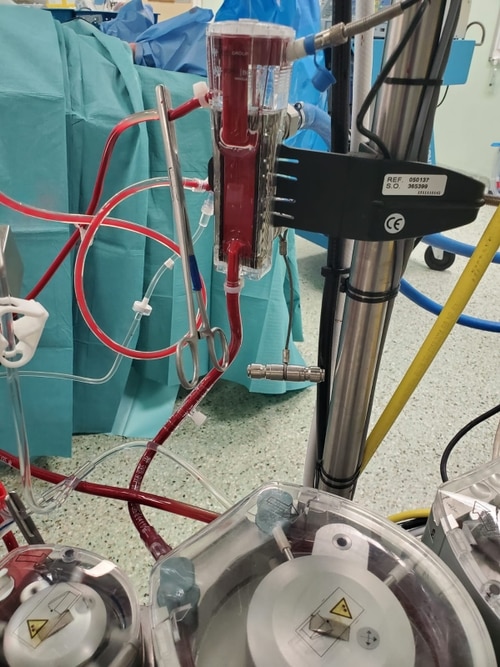
Oxygenator, Heat Exchanger & Arterial Line Filter
The oxygenator is the artificial lung of the bypass circuit. Modern membrane oxygenators consist of thousands of hollow microporous polypropylene fibres (typically 200–300 μm external diameter) bundled within a plastic housing. A gas mixture (oxygen and air, with CO₂ added when needed) flows inside the fibres, while blood flows outside and across them. Oxygen diffuses through the microporous membrane into the blood, whilst carbon dioxide diffuses in the opposite direction and is exhausted through gas outlet ports. Gas exchange efficiency is controlled by adjusting the gas flow rate (sweep) and the fraction of inspired oxygen (FiO₂).
The heat exchanger is an integral component of modern oxygenators, located between the pump and the oxygenator membrane. It consists of stainless steel or polymer tubes through which temperature-controlled water circulates. This allows the perfusionist to cool the patient (for myocardial and cerebral protection) or warm them back to normothermia before weaning from bypass. Temperature gradients are carefully controlled — typically not exceeding a 10°C water-to-blood differential — to prevent gas coming out of solution and forming microbubbles.
The arterial line filter is the final safety barrier before blood re-enters the patient via the arterial cannula. It captures gaseous and particulate microemboli that may have passed through the oxygenator. Most modern oxygenators now integrate the arterial line filter within the device housing, reducing the overall prime volume and surface area of the circuit. This integration helps minimise haemodilution and the inflammatory response associated with extracorporeal circulation.
Cardioplegia
Cardioplegia is a method of myocardial protection and is necessary for the majority of cardiac operations performed on CPB. The technique works by delivering a specialised solution to the heart muscle that electrochemically arrests (stops) the heart in diastole. This dramatically reduces myocardial oxygen consumption — from approximately 8-10 ml O₂/100g/min in a beating heart to approximately 1 ml O₂/100g/min in an arrested, cooled heart — providing critical protection during the period of aortic cross-clamping.
The patient's ascending aorta is clamped with a cross-clamp, isolating the heart from the systemic circulation. Distal to the cross-clamp is the arterial cannula, which delivers oxygenated blood to the body via the heart-lung machine. Proximal to the cross-clamp is the aortic root cannula, through which cardioplegia solution is delivered (antegrade delivery) and through which it can also be vented. Cardioplegia can also be delivered in a retrograde fashion via a catheter placed in the coronary sinus — this is particularly useful when there is significant coronary artery disease that may prevent uniform antegrade distribution.
The aim of cardioplegia is to provide a still, bloodless surgical field whilst protecting the myocardium from ischaemic injury. The solution is given at varying temperatures: cold (4°C) to reduce cellular metabolic demand, and warm (37°C) — often as a terminal "hot shot" — to promote aerobic recovery of the myocardium before removing the aortic cross-clamp.
The most widely used cardioplegia solutions contain a high concentration of potassium (typically 20-30 mmol/L) to produce diastolic arrest by depolarising the cardiac cell membrane. The solution is commonly mixed with the patient's own oxygenated blood at ratios ranging from 1:1 to 1:8 (cardioplegia concentrate to blood). This blood-based approach provides ongoing oxygen delivery and buffering capacity to the myocardium during the arrest period.
Additional substances frequently added to cardioplegia solutions include magnesium (membrane stabilisation), bicarbonate (buffering), mannitol (free radical scavenging and osmotic protection), glutamate and aspartate (metabolic substrates), adenosine (vasodilation), procaine (membrane stabilisation), and calcium (at controlled low concentrations to prevent calcium paradox). After the surgical repair is complete, the cross-clamp is removed, warm blood washes away the cardioplegia solution, potassium is cleared, and normal electrochemical activity returns to the heart.